Philosophy and UHC: The Hidden Connection?
Unfortunately, philosophy tends to be underappreciated in the modern world. You might ask, how do the teachings of ancient philosophers come into play? You might have missed philosophy’s influence over Universal Health Coverage (UHC), with these influences coming from utilitarianism and socialism.
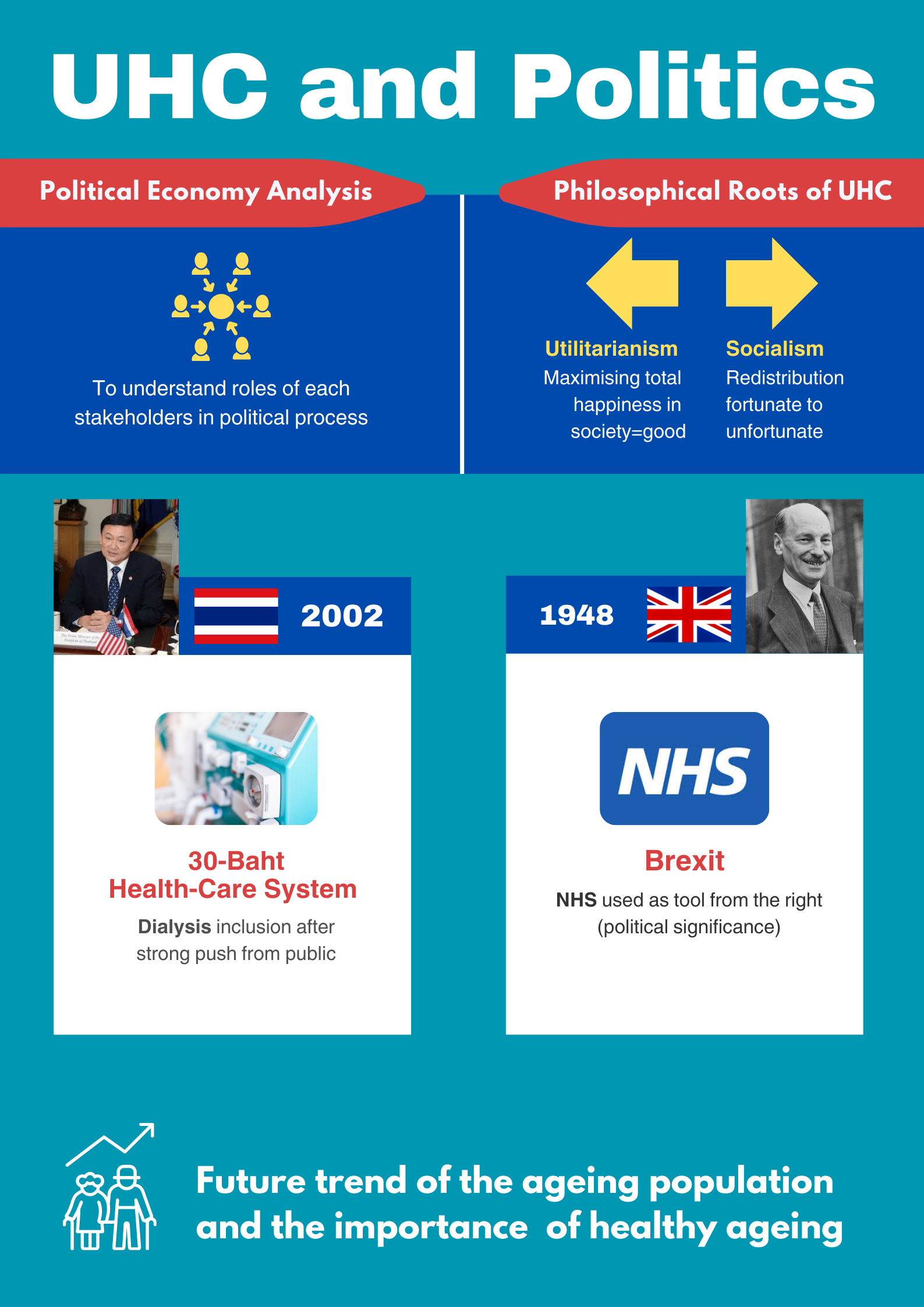
Utilitarianism. This idea states that actions that maximise happiness (and minimise sadness) in a society are the ultimate good. Here, the utility people feel is quantifiable, and any form of action could be justified to maximise this. This is the moral foundation of UHC, which tries to ensure the health of all citizens in a country.
Secondly, the definition of socialism is understandably disputed; ask ten people and they will give ten different answers. At its core, socialism emphasises wealth redistribution from rich to poor, young to old, and healthy to sick—principles that are foundational to UHC. This means higher taxes and larger governments. It is believed to varying degrees that the economy itself (free market) cannot meet societal needs—especially healthcare, which is a perfect example of market failure. This has necessitated governments to step in and play a significant role in ensuring services like healthcare are provided to everyone, regardless of their socioeconomic status.
Political Economy Analysis? What’s That?
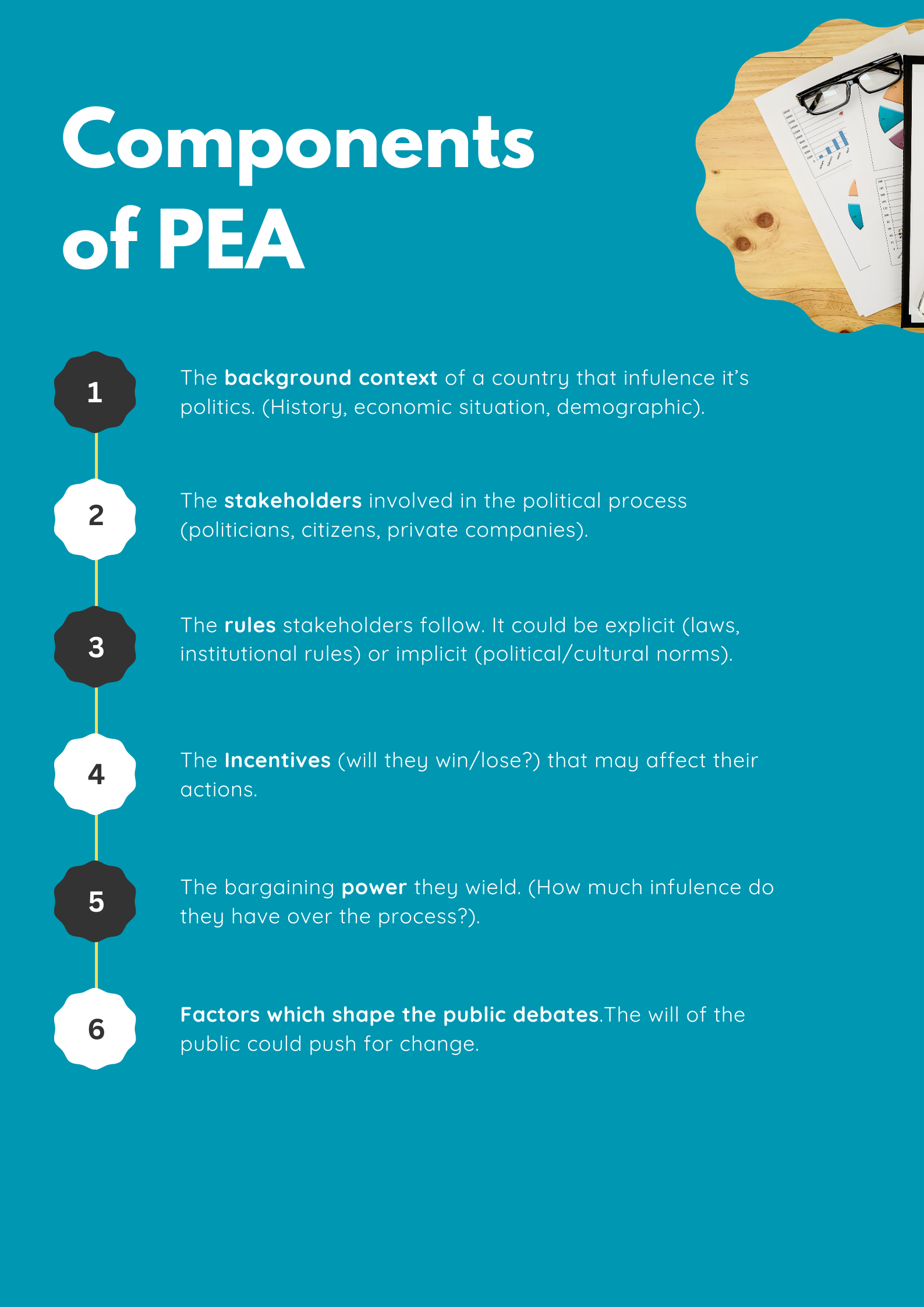
Imagine standing in front of a large, complex machine that you know can do good if it gets working. The machine has numerous connected parts that cohesively work together for functionality. The political process and this complex machine are very alike. Staring at individual parts of the machine will not tell you how the machine works. You need some instructions on how to operate the machine. Similarly, Political Economy Analysis (PEA) is a research framework (like the operating manual for that complex machine) that helps us understand how policies get passed (or not). Understanding the players involved, their roles, and their priorities can help us understand what are the correct buttons to press and the levers to pull to make this machine work and achieve your goals. Through PEA, policymakers and researchers can know who to collaborate with and how to negotiate with those with competing priorities. However, a limitation of carrying out PEA is that it requires inputs from experts with a deep understanding of that political context.
The following graphic illustrates the components of the PEA:
The Birth of UHC—Britain and Thailand
Here’s a quiz for you! Who do you think won the first election in Britain right after WW2?
Churchill? Because he led the UK to victory? Wrong!
The Labour Party won. The explicitly socialist party was led by Clement Attlee, who had an agenda to provide universal healthcare free of charge to the populace; this proved effective. Three years later, in 1948, the National Health Service (NHS) was formed.
The Beveridge Report had a big impact on the formation of the NHS. It was published three years prior, in 1942, and provided a vision for the post-war UK. This vision was very popular among the population, and it sold over 600,000 copies in a year.
Since then, the NHS has withstood turbulent times—especially since the 2010s with the deadly ABCs. A for Austerity, B for Brexit and, you guessed it, C for COVID-19. One could argue that the NHS has never been in a more dire situation than now; over the last decade, the average waiting time for patients ballooned to 14 weeks. This waiting time caused patients to report the lowest rate of satisfaction towards the NHS ever recorded.
In 2001, Thaksin Shinawatra, a charismatic businessman, ran for the Thai general election with policy platforms targeting the poorer rural population. One of his flagship policies was the 30 Baht healthcare scheme, where all Thais would be able to access healthcare by paying 30 Baht.
Aaaaand kaboom! The public loved his proposal and elected him into office. This is how Thailand achieved UHC across all its population by 2002.
The roots of the 30 Baht healthcare scheme could be traced back to the 1997 constitution (which was devised after the coup in 2007). This included the right for all Thais to access healthcare. Thaksin needed popular support in the 2001 election, so he offered the population free healthcare.
In contrast to its British counterpart, the inception of the Thai UHC system may seem less radical. Thailand had fewer ideological roots, and UHC was a pragmatic choice—but there are many similarities too. They both expanded pre-existing systems to cover the whole populace. UHC in both countries was implemented while recovering from a crisis—World War 2 for the UK and the 1997 Asian Financial Crash for Thailand. In addition, it was a representation of sweeping changes made to the country, which involved the implementation of various measures.
Case Studies: How Political Economy Reigns Over Health in the Two Kingdoms
One of the most memorable campaigns in Brexit (short for Britain opting to leave the European Union) was the Brexit bus with the slogan: “We send the EU £350 million a week, let’s fund our NHS instead.” As we can see from the slogan, the NHS was politicised and used as a propaganda tool to sway the British public. In addition, the Brexiteers also claimed that many EU immigrants who use the NHS were causing problems. These campaign claims were made because of the significance of the NHS to the British public. Since Brexit, the pretty painting the Brexiteers drew was destroyed by the dropkick of veteran wrestler El Reality. El Reality has also punched down economic growth in the UK, which, as a result, worsened the health conditions of the British public and the financial situation of the government. Not only that, it made it harder for medical personnel from EU member states to work in the UK.
In Thailand, after facing strong pushback from civil societies and movements by nephrologists, Renal Replacement Therapy (RRT) to treat patients with End-Stage Renal Disease (ESRD) was included in the UHC package in 2008. Despite dialysis not being cost-effective and having a high impact on the National Health Security Office (NHSO) budget, social, economic, and political reasons prevailed. Without UHC, Thai people faced catastrophic healthcare expenditure, risking life below the poverty line, and without RRT, the disease would surely prove fatal. This prompted the government to introduce peritoneal dialysis (PD)—the “PD first” policy.
Through the Crystal Ball: How Will Politics Affect Health in the Future?
In both the UK and Thailand, health expenditure has been increasing year on year. This growth can partly be attributed to an increasing ageing population, which requires more healthcare resources. This is not limited to these two countries, as we can tell from the fact that by 2030 a sixth of the world’s population will be over 60.
This demographic shift will come with a new challenge, where we will have to ensure the well-being of the elderly population while keeping our UHC financially sustainable.
Few countries are already taking a step towards healthy ageing. In 2023, the Singaporean government introduced the “Live Well Age Well” programme, which offers group exercise sessions as part of their initiative.
A Brief Conclusion
Here, I have attempted to connect the dots between health and political economy like a cool detective. This learning journey was full of discoveries and surprises for me too. I hope this blog was an informative and enjoyable read.
Sawadee Krub!